




The outcome of treatment depends on anatomical repositioning of the fracture block, strong fixation of the fracture, preservation of good soft tissue coverage and early functional exercise.
Anatomy
The distal humerus is divided into a medial column and a lateral column (Figure 1).
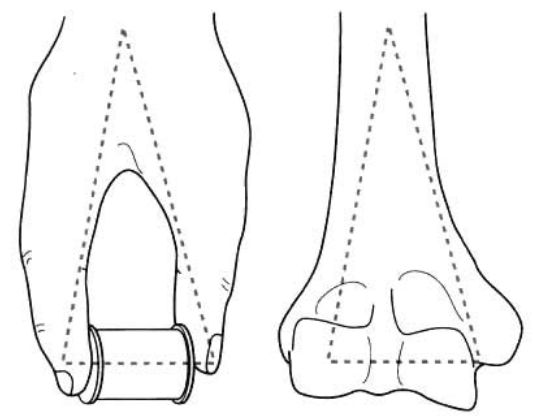
Figure 1 The distal humerus consists of a medial and lateral column
The medial column includes the medial portion of the humeral epiphysis, the medial epicondyle of the humerus and the medial humeral condyle including the humeral glide.
The lateral column comprising the lateral portion of the humeral epiphysis, the external epicondyle of the humerus and the external condyle of the humerus including the humeral tuberosity.
Between the two lateral columns is the anterior coronoid fossa and the posterior humeral fossa.
Injury mechanism
Supracondylar fractures of the humerus are most often caused by falls from high places.
Younger patients with intra-articular fractures are most often caused by high-energy violent injuries, but older patients can have intra-articular fractures from lower-energy violent injuries due to osteoporosis.
Typing
(a)There are supracondylar fractures, condylar fractures and intercondylar fractures.
(b)Supracondylar fractures of the humerus: the fracture site is located above the hawk's fossa.
(c)Humeral condylar fracture: the fracture site is located in the hawk's fossa.
(d)intercondylar fracture of the humerus: the fracture site is located between the distal two condyles of the humerus.
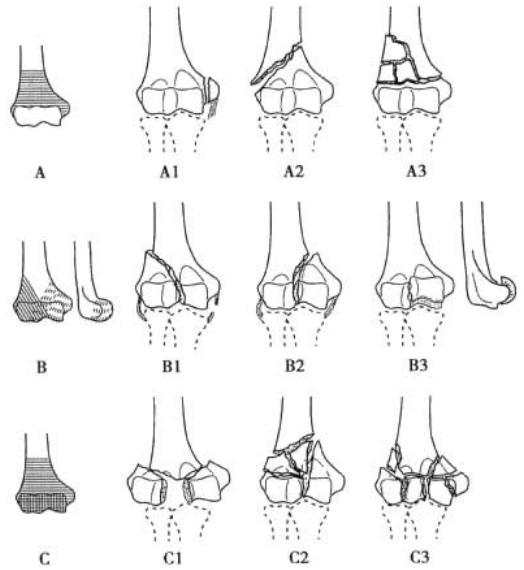
Figure 2 AO typing
AO humeral fracture typing (Figure 2)
Type A: extra-articular fractures.
Type B: fracture involving the articular surface (single-column fracture).
Type C: complete separation of the articular surface of the distal humerus from the humeral stem (bicolumnar fracture).
Each type is further divided into 3 subtypes according to the degree of comminution of the fracture, (1 ~ 3 subtypes with increasing degree of comminution in that order).
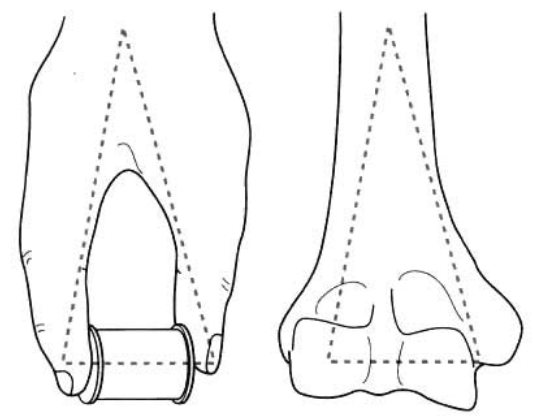
Figure3 Riseborough-Radin typing
Riseborough-Radin typing of intercondylar fractures of the humerus (all types include the supracondylar portion of the humerus)
Type I:fracture without displacement between the humeral tuberosity and the talus.
Type II:intercondylar fracture of the humerus with displacement of the fracture mass of the condyle without rotational deformity.
Type III:intercondylar fracture of the humerus with displacement of the fracture fragment of the condyle with rotational deformity.
Type IV:severe comminuted fracture of the articular surface of one or both condyles (Figure 3).

Figure 4 Type I humeral tuberosity fracture
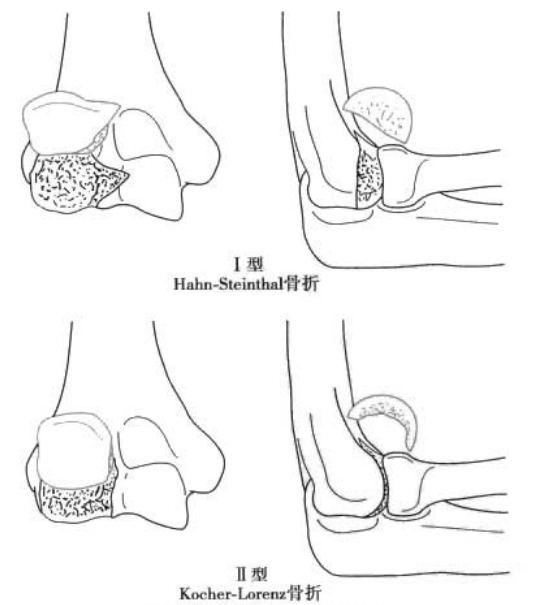
Figure 5 Humeral tuberosity fracture staging
Fracture of the humeral tuberosity: shear injury of the distal humerus
Type I: fracture of the entire humeral tuberosity including the lateral edge of the humeral talus ( Hahn-Steinthal fracture) (Figure 4).
Type II: subchondral fracture of the articular cartilage of the humeral tuberosity ( Kocher-Lorenz fracture).
Type III: comminuted fracture of the humeral tuberosity (Figure 5).
Non-operative treatment
Non-operative treatment methods for distal humeral fractures have a limited role. The aim of non-operative treatment is: early joint movement to avoid joint stiffness; elderly patients, who mostly suffer from multiple compound diseases, should be treated with a simple method of splinting the elbow joint in 60° of flexion for 2-3 weeks, followed by light activity.
Surgical treatment
The aim of treatment is to restore pain-free functional range of motion of the joint (30° of elbow extension, 130° of elbow flexion, 50° of anterior and posterior rotation); firm and stable internal fixation of the fracture allows the start of functional elbow exercises after skin wound healing; double plate fixation of the distal humerus includes: medial and posterior lateral double plate fixation, or medial and lateral double plate fixation.
Surgical method
(a) The patient is placed in an upward lateral position with a liner placed under the affected limb.
identification and protection of the median and radial nerves intraoperatively.
Posterior elbow can be extended surgical access: ulnar hawk osteotomy or triceps retraction to expose deep articular fractures
ulnar hawkeye osteotomy: adequate exposure, especially for comminuted fractures of the articular surface. However, fracture non-union often occurs at the osteotomy site. The fracture non-union rate has been significantly reduced with improved ulnar hawk osteotomy (herringbone osteotomy) and transtension band wire or plate fixation.
Triceps retraction exposure can be applied to distal humeral trifold block fractures with joint comminution, and expanded exposure of the humeral slide can cut off and expose the ulnar hawk tip at about 1 cm.
It has been found that the two plates can be placed orthogonally or in parallel, depending on the type of fracture in which the plates should be placed.
Articular surface fractures should be restored to a flat articular surface and fixed to the humeral stem.
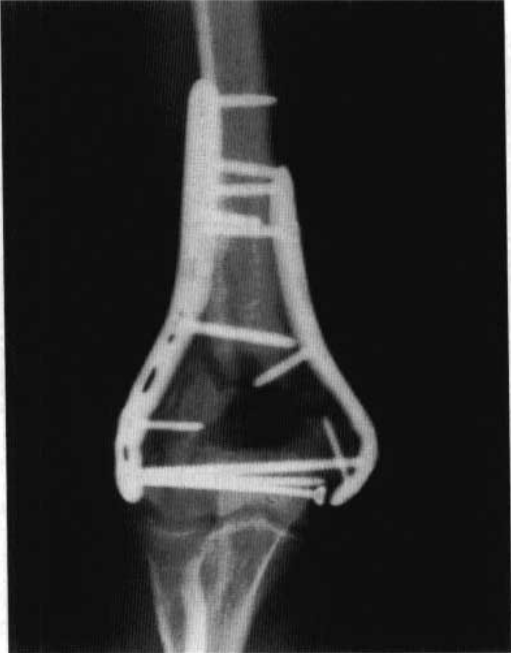
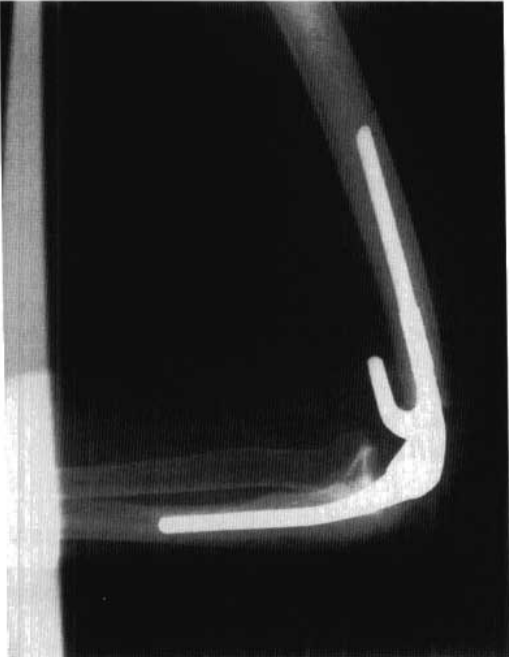
Figure 6 Post-operative internal fixation of elbow fracture
Temporary fixation of the fracture block was performed by applying a K wire, after which the 3.5 mm power compression plate was trimmed to the shape of the plate according to the shape behind the lateral column of the distal humerus, and the 3.5 mm reconstruction plate was trimmed to the shape of the medial column, so that both sides of the plate would fit the bone surface (the new advance shaping plate could simplify the process.) (Figure 6).
Take care not to fix the articular surface fracture fragment with all-threaded cortical screws with pressure from the medial to the lateral side.
the epiphysis-humerus thousand migration site is important to avoid non-union of the fracture.
giving bone graft filling at the site of the bone defect, applying iliac cancellous bone grafts to fill the compression fracture defect: medial column, articular surface and lateral column, grafting cancellous bone to the side with intact periosteum and compression bone defect at the epiphysis.
Remember the key points of fixation.
Fixation of the distal fracture fragment with as many screws as possible.
fixation of as many fragmentary fracture fragments as possible with screws crossing medially to laterally.
Steel plates should be placed on the medial and lateral sides of the distal humerus.
Treatment options: Total elbow arthroplasty
For patients with severe comminuted fractures or osteoporosis, total elbow arthroplasty can restore elbow joint motion and hand function after the less demanding patients; the surgical technique is similar to total arthroplasty for degenerative changes of the elbow joint.
(1) application of a long stem-type prosthesis to prevent proximal fracture extension.
(2) Summary of surgical operations.
(a) The procedure is performed using a posterior elbow approach, with steps similar to those used for distal humeral fracture incision and internal fixation (ORIF).
Anteriorization of the ulnar nerve.
access through both sides of the triceps to remove the fragmented bone (key point: do not cut the stop of the triceps at the ulnar hawk site).
The entire distal humerus including the hawk fossa can be removed and a prosthesis fitted, which will not leave any significant sequelae if an additional I to 2 cm is removed
adjustment of the intrinsic tension of the triceps muscle during the fitting of the humeral prosthesis after excision of the humeral condyle.
Excision of the tip of the proximal ulnar eminence to allow better access for exposure and installation of the ulnar prosthesis component (Figure 7).
Figure 7 Elbow arthroplasty
Postoperative care
Postoperative splinting of the posterior aspect of the elbow joint should be removed once the patient's skin wound heals, and active functional exercises with assistance should be started; the elbow joint should be fixed for a long enough time after total joint replacement to promote skin wound healing (the elbow joint can be fixed in the straight position for 2 weeks after surgery to help obtain better extension function); a removable fixed splint is now commonly used clinically to facilitate range of motion exercises when It can be removed frequently to better protect the affected limb; active functional exercise is usually started 6-8 weeks after the skin wound has completely healed.
Postoperative care
Postoperative splinting of the posterior aspect of the elbow joint should be removed once the patient's skin wound heals, and active functional exercises with assistance should be started; the elbow joint should be fixed for a long enough time after total joint replacement to promote skin wound healing (the elbow joint can be fixed in the straight position for 2 weeks after surgery to help obtain better extension function); a removable fixed splint is now commonly used clinically to facilitate range of motion exercises when It can be removed frequently to better protect the affected limb; active functional exercise is usually started 6-8 weeks after the skin wound has completely healed.
Post time: Dec-03-2022





