




Tibial plateau fractures combined with ipsilateral tibial shaft fractures are commonly seen in high-energy injuries, with 54% being open fractures. Previous studies have found that 8.4% of tibial plateau fractures are associated with concomitant tibial shaft fractures, while 3.2% of tibial shaft fracture patients have concomitant tibial plateau fractures. It is evident that the combination of ipsilateral tibial plateau and shaft fractures is not uncommon.
Due to the high-energy nature of such injuries, there is often severe soft tissue damage. In theory, the plate and screw system has advantages in internal fixation for plateau fractures, but whether the local soft tissue can tolerate the internal fixation with a plate and screw system is also a clinical consideration. Therefore, there are currently two commonly used options for internal fixation of tibial plateau fractures combined with tibial shaft fractures:
1. MIPPO (Minimally Invasive Plate Osteosynthesis) technique with a long plate;
2. Intramedullary nail + plateau screw.
Both options are reported in the literature, but there is currently no consensus on which is superior or inferior in terms of fracture healing rate, fracture healing time, lower limb alignment, and complications. To address this, scholars from a Korean university hospital conducted a comparative study.

The study included 48 patients with tibial plateau fractures combined with tibial shaft fractures. Among them, 35 cases were treated with the MIPPO technique, with lateral insertion of a steel plate for fixation, and 13 cases were treated with plateau screws combined with an infrapatellar approach for intramedullary nail fixation.
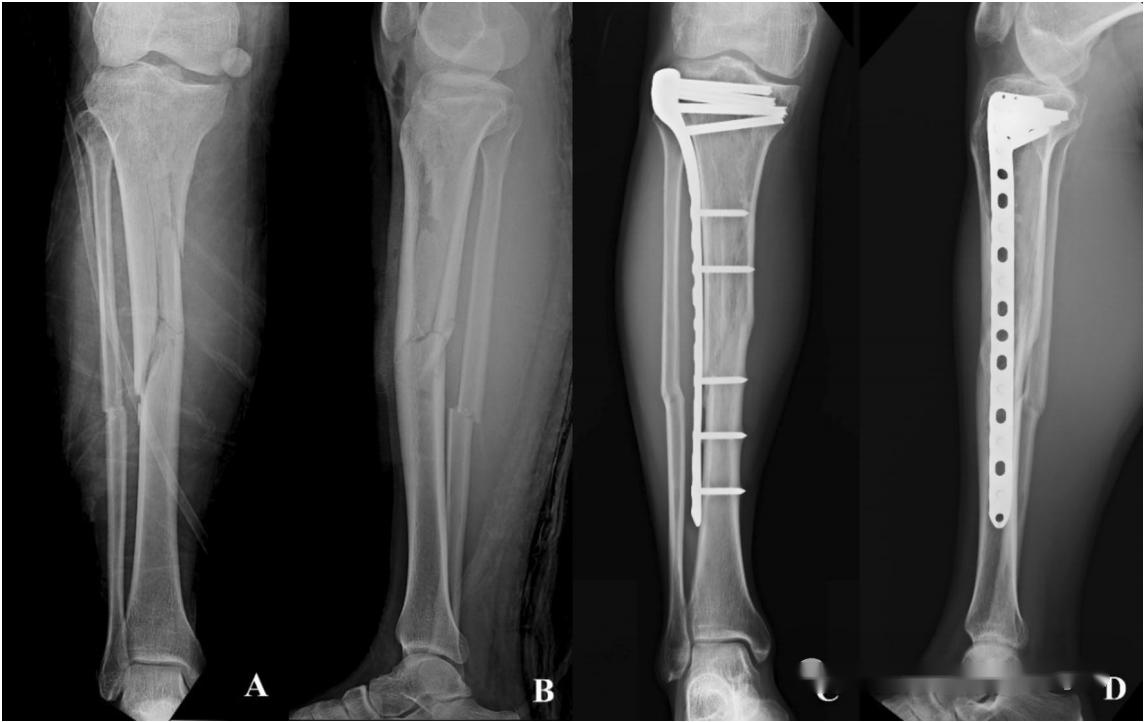
▲ Case 1: Lateral MIPPO steel plate internal fixation. A 42-year-old male, involved in a car accident, presented with an open tibial shaft fracture (Gustilo II type) and a concomitant medial tibial plateau compression fracture (Schatzker IV type).
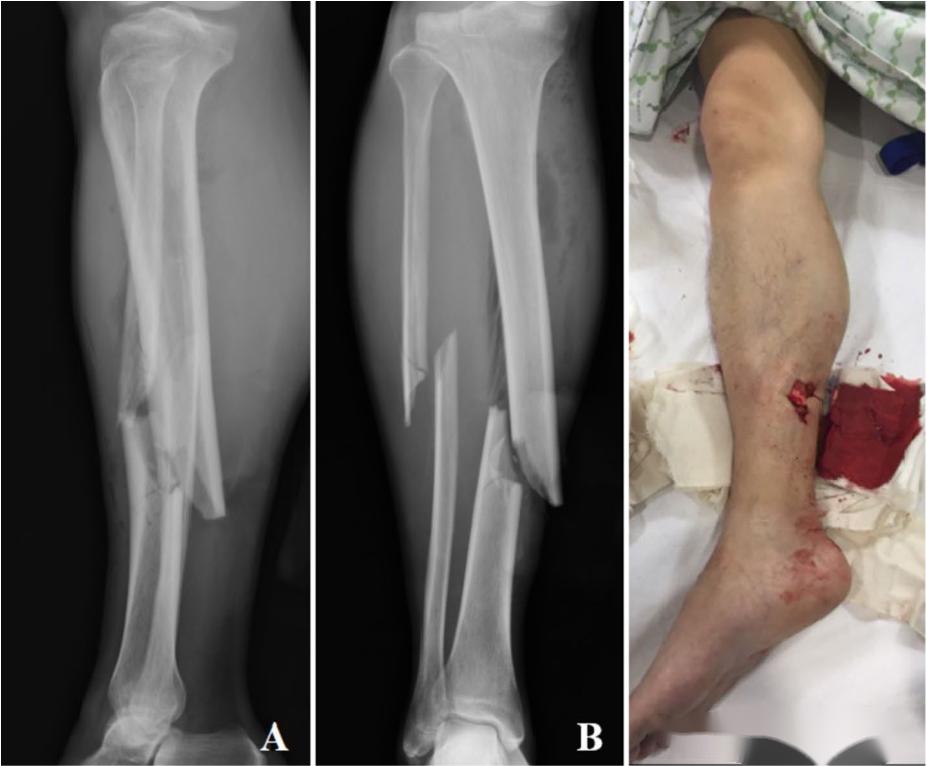
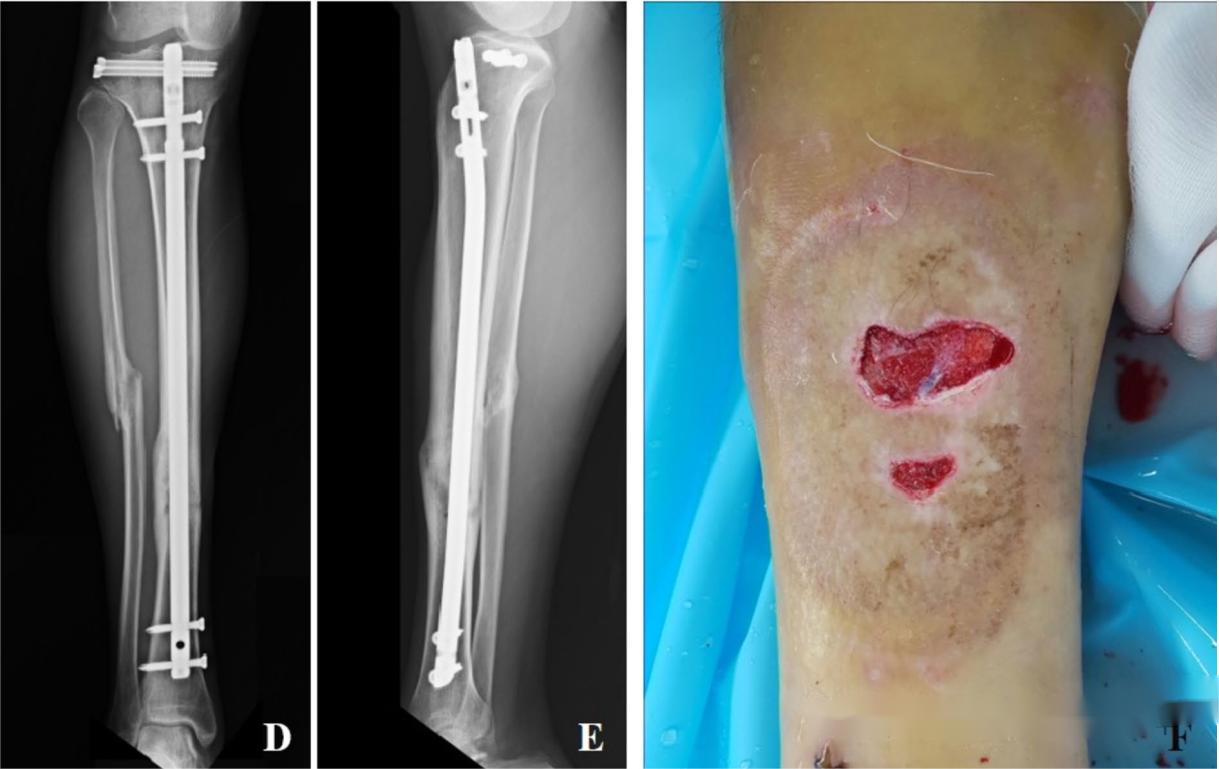
▲ Case 2: Tibial plateau screw + suprapatellar intramedullary nail internal fixation. A 31-year-old male, involved in a car accident, presented with an open tibial shaft fracture (Gustilo IIIa type) and a concomitant lateral tibial plateau fracture (Schatzker I type). After wound debridement and negative pressure wound therapy (VSD), the wound was skin grafted. Two 6.5mm screws were used for reduction and fixation of the plateau, followed by intramedullary nail fixation of the tibial shaft via a suprapatellar approach.
The results indicate that there is no statistically significant difference between the two surgical approaches in terms of fracture healing time, fracture healing rate, lower limb alignment, and complications.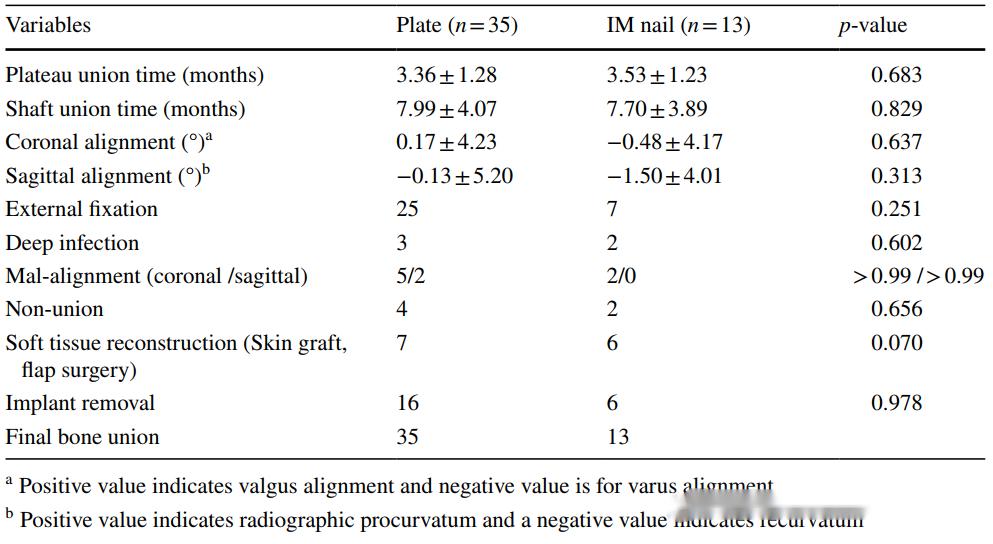
Similar to the combination of tibial shaft fractures with ankle joint fractures or femoral shaft fractures with femoral neck fractures, high-energy-induced tibial shaft fractures can also lead to injuries in the adjacent knee joint. In clinical practice, preventing misdiagnosis is a primary concern in diagnosis and treatment. Additionally, in the choice of fixation methods, although current research suggests no significant differences, there are still several points to consider:
1. In cases of comminuted tibial plateau fractures where simple screw fixation is challenging, priority may be given to the use of a long plate with MIPPO fixation to adequately stabilize the tibial plateau, restoring joint surface congruence and lower limb alignment.
2. In cases of simple tibial plateau fractures, under minimally invasive incisions, effective reduction and screw fixation can be achieved. In such cases, priority may be given to screw fixation followed by suprapatellar intramedullary nail fixation of the tibial shaft.
Post time: Mar-09-2024





