




KEYPOINT
1. The unipolar electric knife cuts the fascia and then peels the muscle under the periosteum, pay attention to protect the articular synovial joint, meanwhile the ligament at the root of the spinous process should not be removed in order to keep the integrity of the cervical tension band;
2. Pay attention to the gradual increase of the opening of the door as a whole, two small spatulas can be used to open a small portion of one vertebral plate and then the other one, and so on repeatedly, and gradually open it to the ideal width (the spinal canal is enlarged by 4mm), which can avoid complete fracture of the slotted side to the maximum extent possible;
3. When opening the door unilaterally, biting off the ligamentum flavum at the opening site may lead to bleeding from the venous plexus, at this time, do not panic, you can apply bipolar electrocoagulation to stop the bleeding, or gelatin sponges to stop the bleeding.
OPEN-DOOR Posterior cervical spine surgery was first invented by Japanese scholars in the 1970s. Although it has been improved many times, the basic surgical operation is still more or less the same, which is relatively more convenient and similar to the posterior double-door operation with similar therapeutic effect, and it is one of the classic cervical spine surgery for spine surgeons.
1.OPEN-DOOR Expansile Cervical Laminoplasty
This article is from the Department of Neurological Surgery at the University of Miami Hospital in Miami, Florida, and in terms of the specific choice of procedure, they chose an open-door procedure from C3 to C7 for most patients, while applying allograft ribs propped open to the open-door site and supplemented with autologous implants, as described below:
The patient was placed in the prone position, the head was fixed with Mayfield head frame, the tape was used to pull down the patient's shoulder and fix it on the operating bed, 1% lidocaine and epinephrine were used for local infiltration and then the skin was incised along the midline to reach the fascia, and the muscles were peeled off from under the periosteum after incision of the fascia with a single-stage electrosurgical knife, and the protection of articular synovial joints was paid attention to, and the ligament of the sphenoidal root should not be resected in order to keep the integrity of the tension band of the cervical vertebrae; the upper and lower exposures were made. The upper and lower exposure ranges reached the lower part of the C2 vertebral plate and the upper part of the T1 vertebral plate, and the lower third of the C2 vertebral plate and the upper third of the T1 vertebral plate were removed with a grinding drill, and then the ligamentum flavum was cleaned up by a 2-mm plate biting forceps to expose the dura mater, and part of the spinous process was bitten by a biting forceps to prepare for the implantation of the bone.
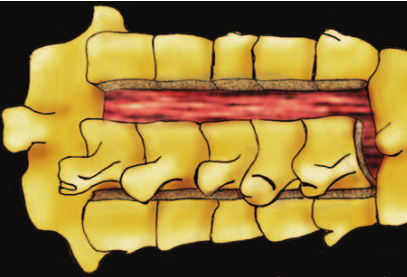
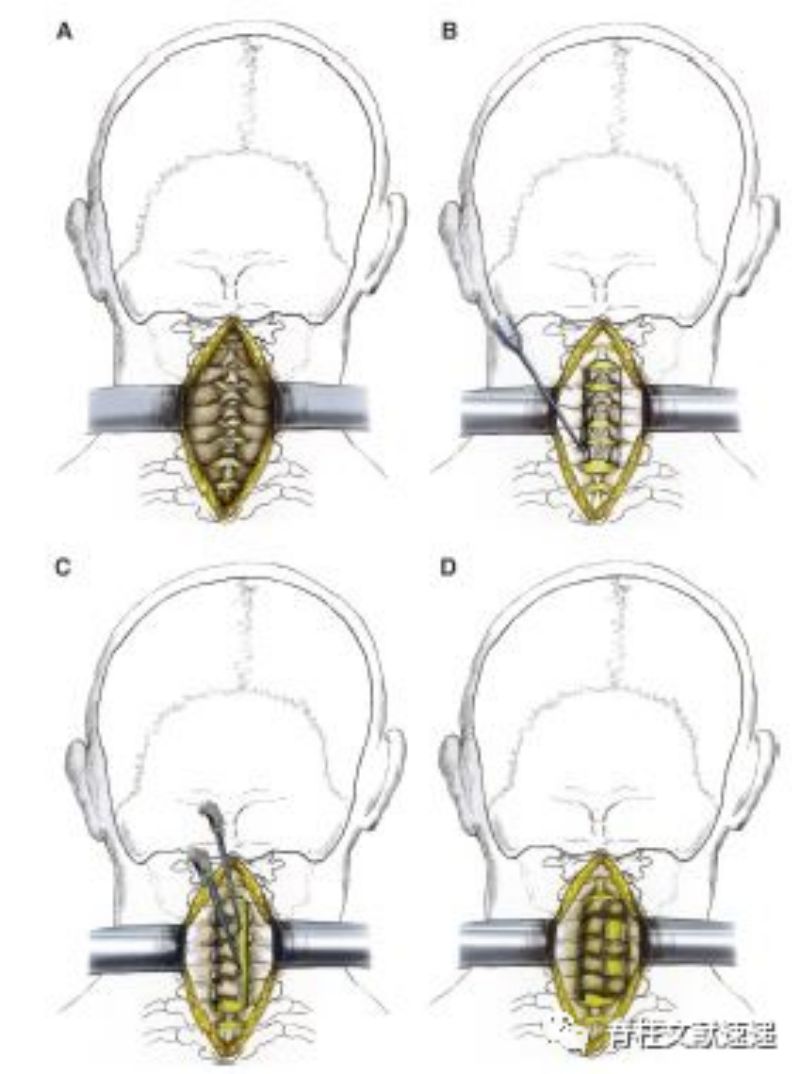
Next the C3-C7 door opening was performed, as shown in the figure above, in general the side with the heavier symptoms was used as the door opening side and the lighter side was used as the hinge, the door opening or slotting site was in the junction area of the vertebral plate and articular eminence, the door opening side was ground through the cortex bilaterally and the hinge side was ground through the cortex in a single layer, and a match head grinding head was used for the door opening.
After grinding through the cortex bilaterally, the open side of the door needs to be cleaned up with the ligamentum flavum with a vertebral plate biting forceps until the dural sac can be clearly seen, and then use a small spatula to pry open the "door" to about 8-16mm and put in the implant block, paying attention to the gradual increase of the overall size of the open door, and the two small spatulas can be used to open up one vertebral plate for a small amount before opening up the other, and then repeating the process, and then opening up the door gradually to the ideal width (the canal widens by 4mm), and in this way, it can be avoided to avoid the complete fracture on the side of the slots to the maximum extent possible.
There should be a slight presence of compressive stress at the site where the bone block is placed without the need for external fixation, and the authors have seen very few complications in the clinic where the bone block falls into the spinal canal, with the final implantation of the bone removed from the spinous process on the hinge side.
2.OPEN-DOOR Cervical Expansile Laminoplasty
This article, from the Department of Neurosurgery at Keck Medical Center of the University of Southern California, has almost the same title as the previous document, with a change in the order of the English words, and a high degree of consistency in its method and philosophy of operation, and reflects the uniformity in the training of surgeons in the United States.
Surgical segments were almost exclusively C3-7 to facilitate posterior displacement of the spinal cord; sphenoidal root ligaments were preserved to facilitate cervical stability; a match head milling drill was used to open the door to minimise damage to the spinal cord; and bone blocks were placed at C3, 5, and 7 to support the opening of the door.
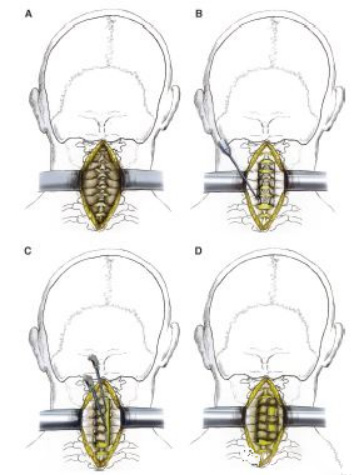
Figure Note: A, Exposure of the lamina from the bottom of C2 to the top of T1. b, Drilling of the lateral groove with a complete osteotomy on one side and a partial osteotomy on the other side. c, Elevation of the lamina from C3 to C7 as a single unit. d, Placement of an allograft bone spacer.
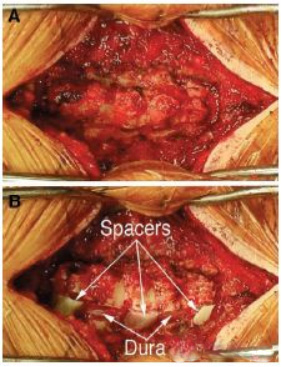
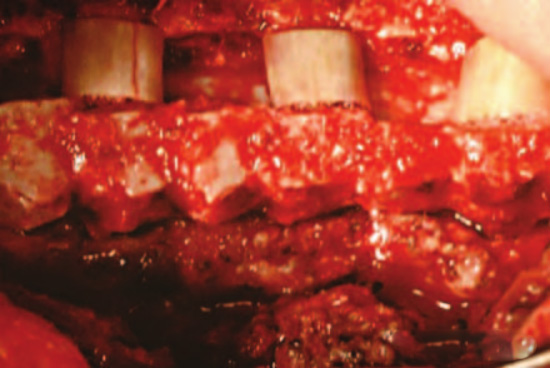
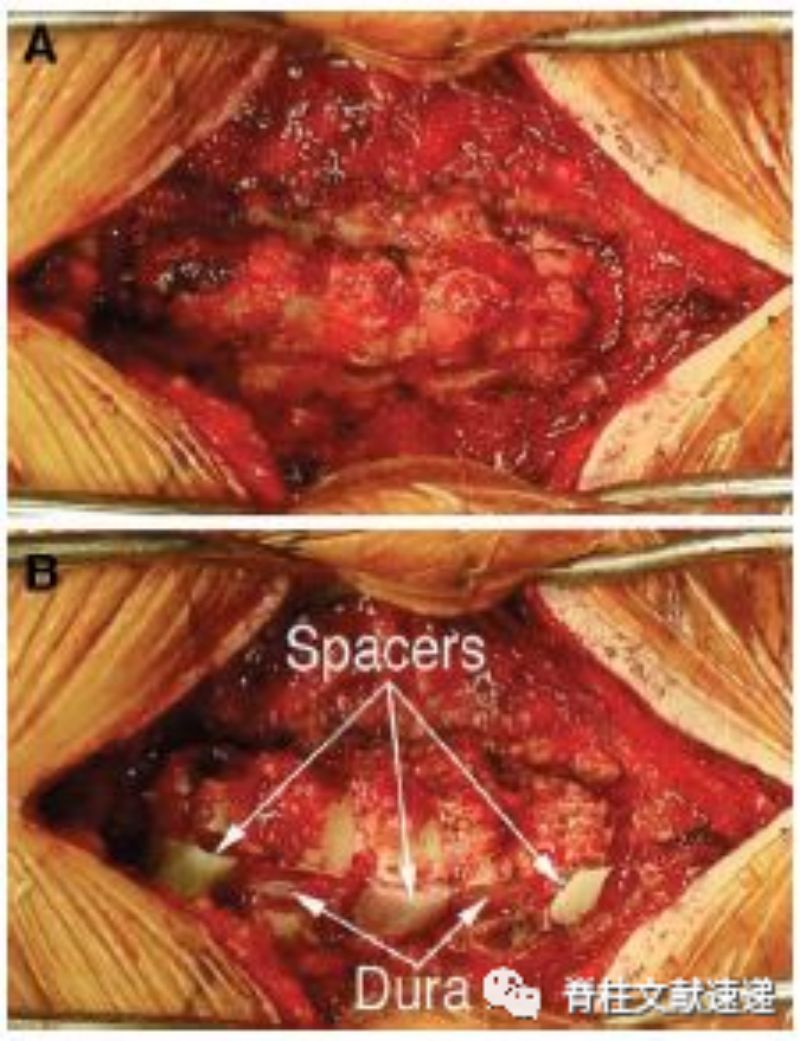
Figure Note: Intraoperative view after drilling holes in the lateral grooves of C3, C5, and C7 (A) and after placement of an allograft rib spacer (B).
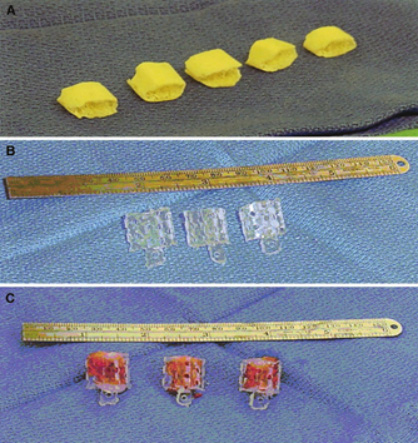
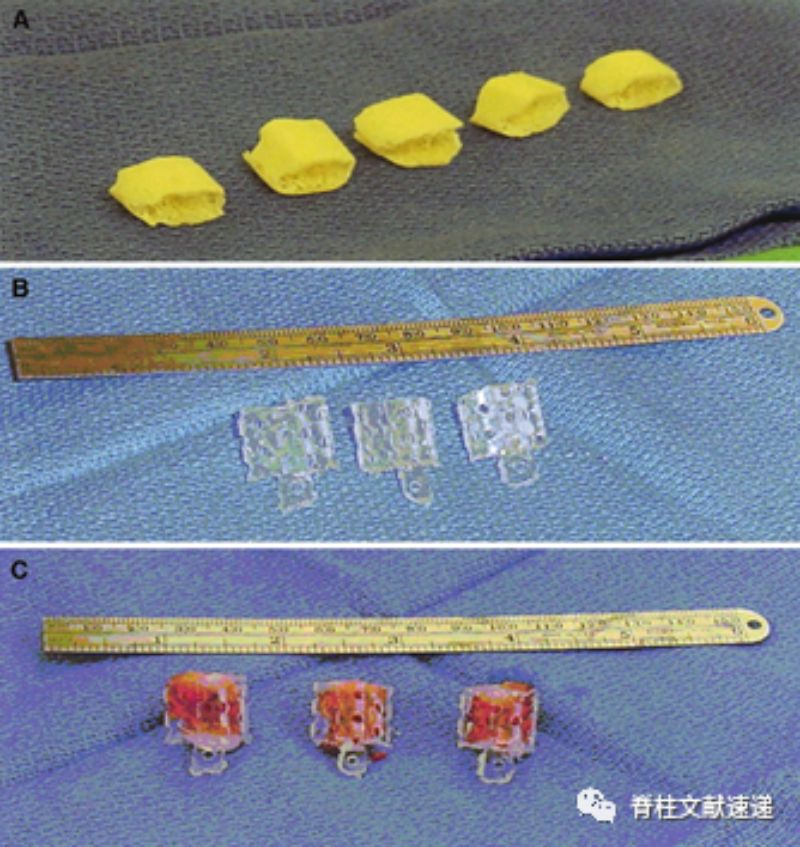
However, its bone graft material, in addition to allogeneic bone (Fig. A), is a vertebral autogenous bone graft made of polylactic acid mesh, as shown below (BC Fig.), which is less common in China. In terms of the width of the door opening, the ideal width is considered to be 10-15 mm, which is slightly different from the 8-16 mm above.
When performing a single door opening of the vertebral plate, biting off the ligamentum flavum at the site of the door opening may result in bleeding from the vein, at this time do not panic, you can apply bipolar electrocoagulation to stop the bleeding or gelatin sponge to stop the bleeding.
3.Cervical Laminoplasty
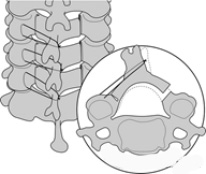
In addition to supporting the bone block at the door opening, other methods of fixing the door opening are described in this article, such as the tie-wire method and the microplates fixation method, the latter of which is currently more commonly used in clinical practice and provides a secure fixation.

Reference
1.Elizabeth V , Sheth R N , Levi A D . OPEN-DOOR EXPANSILE CERVICAL LAMINOPLASTY[J]. Neurosurgery(suppl_1):suppl_1.
[PMID:17204878;https://www.ncbi.nlm./pubmed/17204878]
2.Wang M Y , Green B A . Open-door Cervical Expansile Laminoplasty[J]. Neurosurgery(1):1.
[PMID:14683548;https://www.ncbi.nlm./pubmed/14683548 ]
3.Steinmetz M P , Resnick D K . Cervical laminoplasty[J]. The Spine Journal, 2006, 6(6 Suppl):274S-281S.
[PMID:17097547;https://www.ncbi.nlm./pubmed/17097547]
Post time: Feb-27-2024






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}