




Femoral neck fracture is a common and potentially devastating injury for orthopaedic surgeons, due to the fragile blood supply, the incidence of fracture non-union and osteonecrosis is higher, the optimal treatment for femoral neck fracture is still controversial, most scholars believe that patients over 65 years of age can be considered for arthroplasty, and patients under the age of 65 years of age can be selected for internal fixation surgery, and the most serious impact on blood flow is caused by the subcapsular type fracture of femoral neck. Subcapital fracture of femoral neck has the most serious haemodynamic impact, and closed reduction and internal fixation is still the routine treatment method for subcapital fracture of femoral neck. Good reduction is conducive to stabilising the fracture, promoting fracture healing and preventing femoral head necrosis.
The following is a typical case of femoral neck subcapital fracture to discuss how to perform closed-displacement internal fixation with cannulated screw.
Ⅰ Basic information of the case
Patient information: male 45 years old
Complaint: left hip pain and activity limitation for 6 hours.
History: The patient fell down while taking a bath, causing pain in the left hip and limitation of activity, which could not be relieved by resting, and was admitted to our hospital with a fracture of the neck of the left femur on radiographs, and was admitted to the hospital in a clear state of mind and poor spirit, complaining of pain in the left hip and limitation of activity, and had not eaten and had not relieved himself of his second bowel movement after the injury.
Ⅱ Physical Examination (Whole Body Check & Specialist Check)
T 36.8°C P87 beats/min R20 beats/min BP135/85mmHg
Normal development, good nutrition, passive position, clear mentality, co-operative in examination. Skin colour is normal, elastic, no oedema or rash, no enlargement of superficial lymph nodes in the whole body or local area. Head size, normal morphology, no pressure pain, mass, hair shiny. Both pupils are equal in size and round, with sensitive light reflex. The neck was soft, the trachea was centred, the thyroid gland was not enlarged, the chest was symmetrical, respiration was slightly shortened, there was no abnormality on cardiopulmonary auscultation, the heart boundaries were normal on percussion, the heart rate was 87 beats/min, the heart rhythm was Qi, the abdomen was flat and soft, there was no pressure pain or rebound pain. The liver and spleen were not detected, and there was no tenderness in the kidneys. The anterior and posterior diaphragms were not examined, and there were no deformities of the spine, upper limbs and right lower limbs, with normal movement. Physiological reflexes were present in the neurological examination and pathological reflexes were not elicited.
There was no obvious swelling of the left hip, obvious pressure pain at the midpoint of the left groin, shortened external rotation deformity of the left lower limb, left lower limb longitudinal axis tenderness (+), left hip dysfunction, sensation and activity of the five toes of the left foot were OK, and the dorsal arterial pulsation of the foot was normal.
Ⅲ Auxiliary examinations
X-ray film showed: left femoral neck subcapital fracture, dislocation of the broken end.
The rest of the biochemical examination, chest X-ray, bone densitometry, and colour ultrasound of the deep veins of the lower limbs did not show any obvious abnormality.
Ⅳ Diagnosis and differential diagnosis
According to the patient's history of trauma, left hip pain, activity limitation, physical examination of the left lower limb shortening external rotation deformity, groin tenderness obvious, the left lower limb longitudinal axis kowtow pain (+), the left hip dysfunction, combined with the X-ray film can be clearly diagnosed. The fracture of trochanter can also have hip pain and activity limitation, but usually the local swelling is obvious, the pressure point is located in the trochanter, and the external rotation angle is larger, so it can be differentiated from it.
Ⅴ Treatment
Closed reduction and hollow nail internal fixation was performed after complete examination.
The preoperative film is as follows


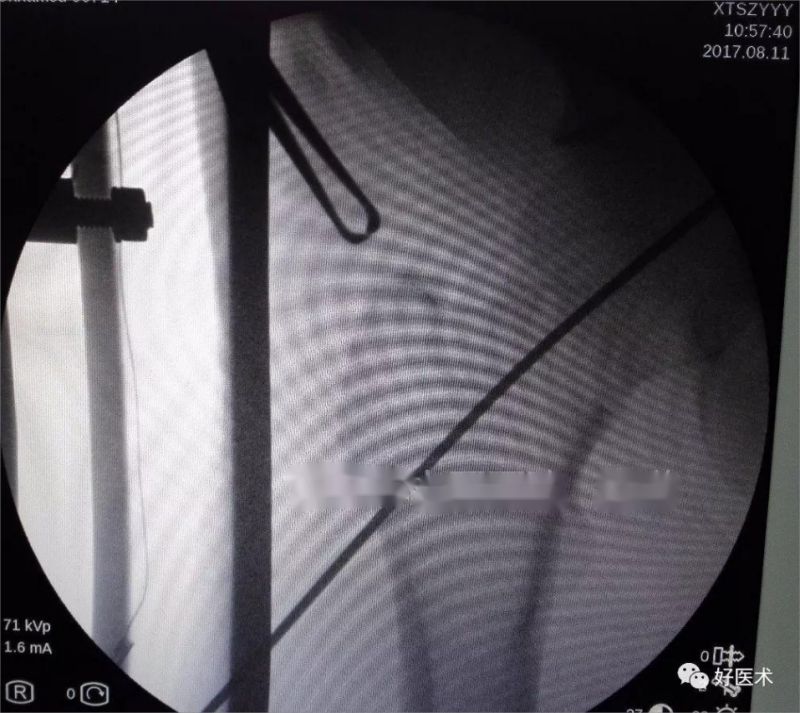
Manoeuvre with internal rotation and traction of the affected limb with a slight abduction of the affected limb after restoration and fluoroscopy showed a good restoration

A Kirschner pin was placed on the surface of the body in the direction of the femoral neck for fluoroscopy, and a small skin incision was made according to the location of the end of the pin.

A guide pin is inserted into the femoral neck parallel to the body surface in the direction of the Kirschner pin while maintaining an anterior tilt of approximately 15 degrees and fluoroscopy is performed
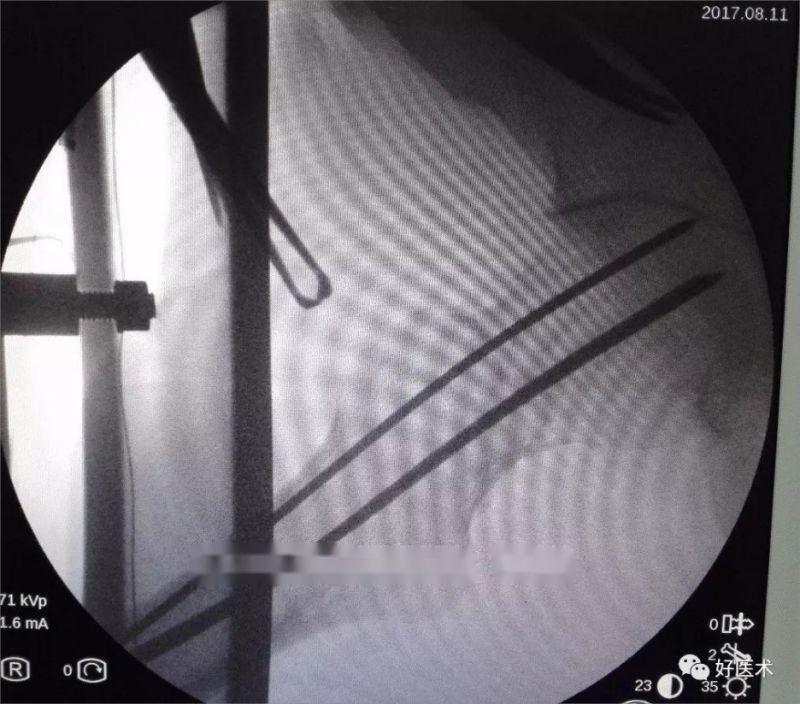
The second guide pin is inserted through the femoral spur using a guide parallel to the underside of the direction of the first guide pin.

A third needle is inserted parallel to the back of the first needle via the guide.
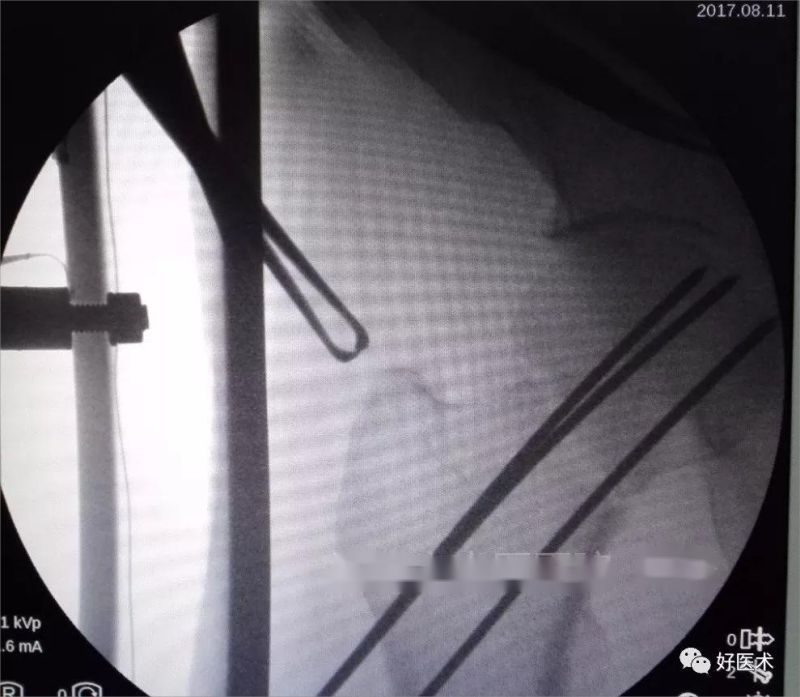
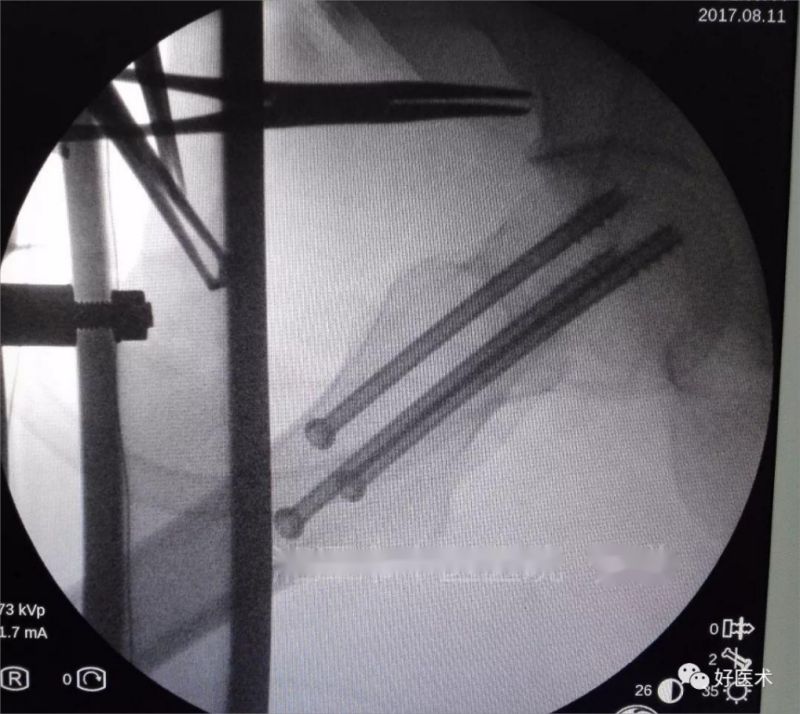
Using a frog fluoroscopic lateral image, all three Kirschner pins were seen to be within the femoral neck
Drill holes in the direction of the guide pin, measure the depth and then select the appropriate length of the hollow nail screwed along the guide pin, it is recommended to screw in the femoral spine of the hollow nail first, which can prevent the loss of reset.
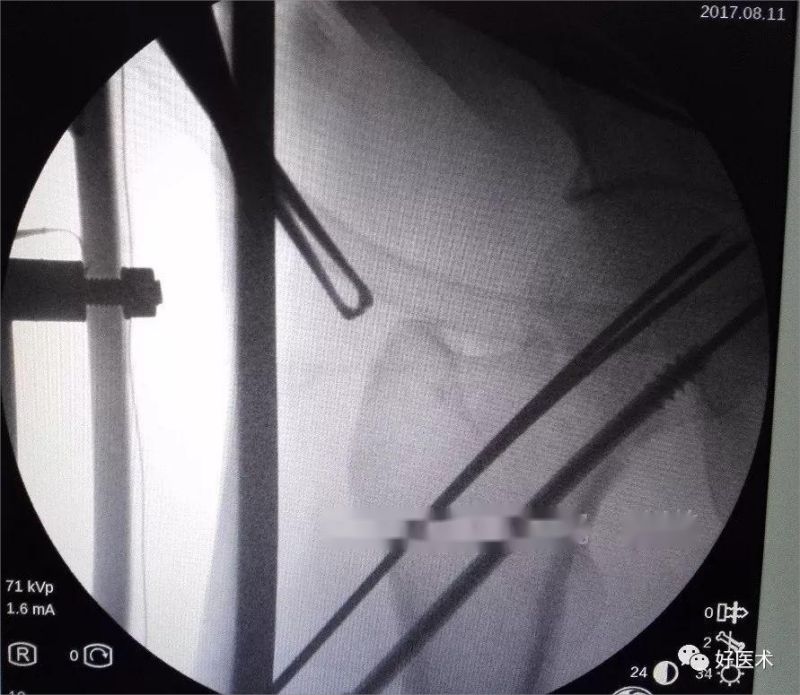
Screw in the other two cannulated screw one after the other and see through the
Skin incision condition

Postoperative review film


Combined with the patient's age, fracture type, and bone quality, closed reduction hollow nail internal fixation was preferred, which has the advantages of small trauma, sure fixation effect, simple operation and easy to master, can be powered compression, hollow structure is conducive to intracranial decompression, and the fracture healing rate is high.
Summary
1 The placement of Kirschner's needles on the body surface with fluoroscopy is conducive to determining the point and direction of needle insertion and the range of skin incision;
2 The three Kirschner's pins should be as parallel, inverted zigzag, and close to the edge as possible, which is conducive to fracture stabilisation and later sliding compression;
3 The bottom Kirschner pin entry point should be selected at the most prominent lateral femoral crest to ensure that the pin is in the middle of the femoral neck, while the tips of the top two pins can be slid forward and backward along the most prominent crest to facilitate the adherence;
4 Don't drive the Kirschner pin too deep at one time to avoid penetrating the articular surface, the drill bit can be drilled through the fracture line, one is to prevent drilling through the femoral head, and the other is conducive to the hollow nail compression;
5 The hollow screws screwed into the almost and then through a little, judge the length of the hollow screw is accurate, if the length is not too far, try to avoid frequent replacement of screws, if osteoporosis, replacement of screws basically become invalid fixation of screws, for the patient's prognosis of effective fixation of screws, but length of the length of the screws is just a little bit worse than the length of ineffective fixation of the screws is much better!
Post time: Jan-15-2024





