




There are two types of surgical methods, plate screws and intramedullary pins, the former includes general plate screws and AO system compression plate screws, and the latter includes closed and open retrograde or retrograde pins. The choice is based on the specific site and type of fracture.
Intramedullary pin fixation has the advantages of small exposure, less stripping, stable fixation, no need for external fixation, etc. It is suitable for middle 1/3, upper 1/3 femur fracture, multi-segmental fracture, pathological fracture. For the lower 1/3 fracture, due to the large medullary cavity and many cancellous bone, it is difficult to control the rotation of intramedullary pin, and the fixation is not secure, although it can be strengthened with screws, but it is more suitable for steel plate screws.
I Open-internal Fixation for Fracture of Femur Shaft with Intramedullary Nail
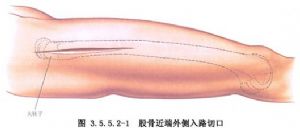
(1) Incision: A lateral or posterior lateral femoral incision is made centred on the fracture site, with a length of 10-12 cm, cutting through the skin and the broad fascia and revealing the lateral femoral muscle.
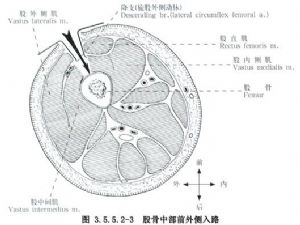
The lateral incision is made on the line between the greater trochanter and the lateral condyle of the femur, and the skin incision of the posterior lateral incision is the same or slightly later, with the main difference being that the lateral incision splits the vastus lateralis muscle, while the posterior lateral incision enters the posterior interval of the vastus lateralis muscle through the vastus lateralis muscle.(Fig 3.5.5.2-1,3.5.5.2-2)。

The anterolateral incision, on the other hand, is made through the line from the anterior superior iliac spine to the outer edge of the patella, and is accessed through the lateral femoral muscle and rectus femoris muscle, which may injure the intermediary femoral muscle and nerve branches to the lateral femoral muscle and branches of the rotator femoris externus artery, and is therefore rarely or never used (Fig 3.5.5.2-3)。
(2) Exposure: Separate and pull the lateral femoral muscle forward and enter it at its interval with the biceps femoris, or directly cut and separate the lateral femoral muscle, but bleeding is more. Cut the periosteum to reveal the upper and lower broken ends of the femur fracture, and reveal the scope to the extent that it can be observed and restored, and strip the soft tissues as little as possible.
(3)Repairing the internal fixation: Adduct the affected limb, expose the proximal broken end, insert the plum blossom or V-shaped intramedullary needle, and try to measure whether the thickness of the needle is appropriate. If there is a narrowing of the medullary cavity, the medullary cavity expander can be used to properly repair and expand the cavity, so as to prevent the needle from not being able to enter and not being able to be pulled out. Fix the proximal broken end with a bone holder, insert the intramedullary needle retrogradely, penetrate the femur from the greater trochanter, and when the end of the needle pushes up the skin, make a small incision of 3cm at the place, and continue to insert the intramedullary needle until it is exposed outside the skin. The intramedullary needle is withdrawn, redirected, passed through the foramen from the greater trochanter, and then inserted proximally to the plane of the cross-section. Improved intramedullary needles have small rounded ends with extraction holes. Then there is no need to pull out and change the direction, and the needle can be punched out and then punched in once. Alternatively, the needle can be inserted retrograde with a guide pin and exposed outside the greater trochanteric incision, and then the intramedullary pin can be inserted into the medullary cavity.
Further restoration of the fracture. Anatomical alignment can be achieved by using the leverage of the proximal intramedullary pin in conjunction with bone pry pivoting, traction, and fracture topping. Fixation is achieved with a bone holder, and the intramedullary pin is then driven so that the pin's extraction hole is directed posteriorly to conform to the femoral curvature. The end of the needle should reach the appropriate part of the distal end of the fracture, but not through the cartilage layer, and the end of the needle should be left 2cm outside of the trochanter, so that it can be removed later.(Fig 3.5.5.2-4)。
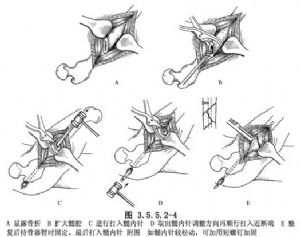
After fixation, try passive movement of the limb and observe any instability. If it is necessary to replace the thicker intramedullary needle, it can be removed and replaced. If there is a slight loosening and instability, a screw can be added to strengthen the fixation.(Fig 3.5.5.2-4)。
The wound was finally flushed and closed in layers. An anti-external rotation plaster boot is put on.
II Plate Screw Internal Fixation
Internal fixation with steel plate screws can be used in all parts of the femoral stem, but the lower 1/3 is more suitable for this type of fixation due to the wide medullary cavity. General steel plate or AO compression steel plate can be used. The latter is more solid and firmly fixed without external fixation. However, neither of them can avoid the role of stress masking and conform to the principle of equal strength, which needs to be improved.
This method has a larger peeling range, more internal fixation, affecting healing, and also has shortcomings.
When there is a lack of intramedullary pin conditions, old fracture medullary curvature or a large part of the impassable and the lower 1/3 of the fracture are more adaptable.
(1)Lateral femoral or posterior lateral incision.
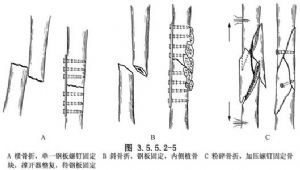
(2)(2) Exposure of the fracture, and depending on the circumstances, it should be adjusted and internally fixed with plate screws. The plate should be placed on the lateral tension side, the screws should pass through the cortex on both sides, and the length of the plate should be 4-5 times of the diameter of the bone at the fracture site. The length of the plate is 4 to 8 times the diameter of the fractured bone. 6 to 8 hole plates are commonly used in the femur. Large comminuted bone fragments can be fixed with additional screws, and a large number of bone grafts can be placed at the same time on the medial side of the comminuted fracture.(Fig 3.5.5.2-5)。
Rinse and close in layers. Depending on the type of plate screws used, it was decided whether or not to apply external fixation with plaster.
Post time: Mar-27-2024





