




Clavicle fractures are one of the most common upper limb fractures in clinical practice, with 82% of clavicle fractures being midshaft fractures. Most clavicle fractures without significant displacement can be treated conservatively with figure-of-eight bandages, while those with significant displacement, interposed soft tissue, risk of vascular or neurological compromise, or high functional demands may require internal fixation with plates. The nonunion rate after internal fixation of clavicle fractures is relatively low, approximately 2.6%. Symptomatic nonunions typically require revision surgery, with the mainstream approach being cancellous bone grafting combined with internal fixation. However, managing recurrent atrophic nonunions in patients who have already undergone nonunion revision is extremely challenging and remains a dilemma for both physicians and patients.
To address this issue, a professor at the Xi'an Red Cross Hospital innovatively used autologous iliac bone structural grafting combined with autologous cancellous bone grafting to treat refractory nonunions of clavicle fractures following failed revision surgery, achieving favorable outcomes. The research results were published in the journal "International Orthopaedics".
Surgical procedure
The specific surgical procedures can be summarized as the figure below:
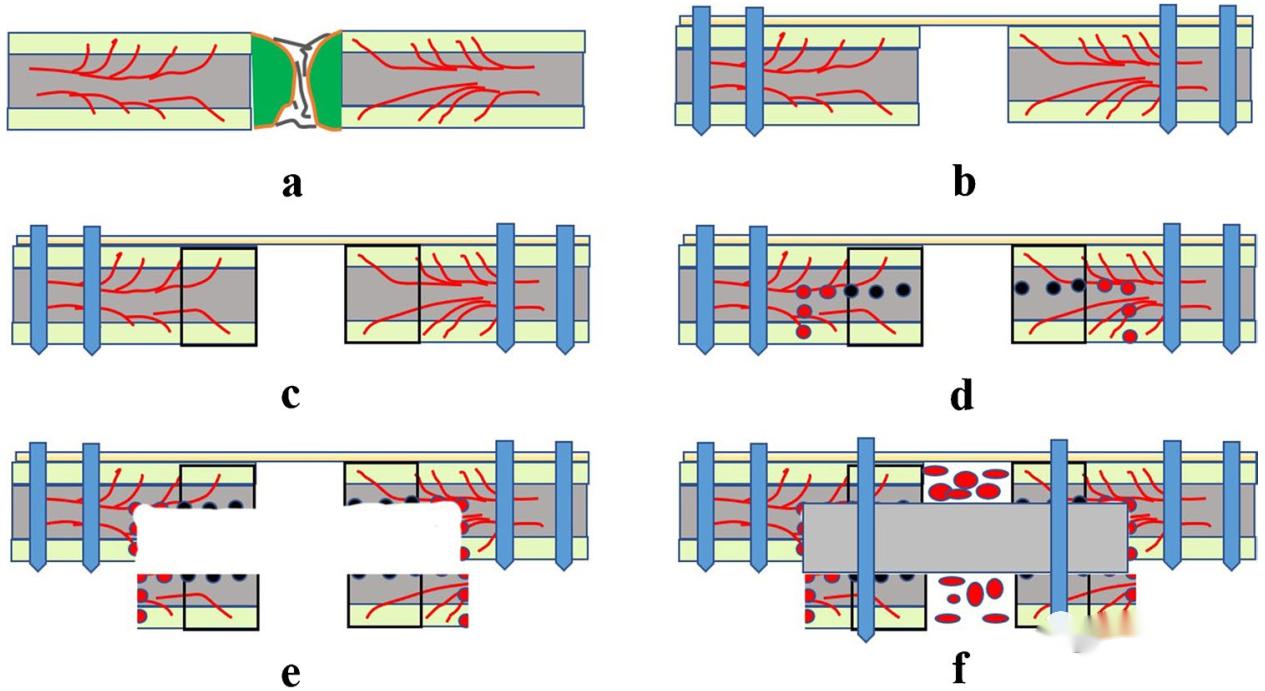
a: Remove the original clavicular fixation, remove the sclerotic bone and fiber scar at the broken end of the fracture;
b: Plastic clavicle reconstruction plates were used, locking screws were inserted into the inner and outer ends to maintain the overall stability of the clavicle, and screws were not fixed in the area to be treated at the broken end of the clavicle.
c: After plate fixation, drill holes with Kirschler needle along the broken end of the fracture to the inside and outside until the hole oozed blood (red pepper sign), indicating good bone blood transport here;
d: At this time, continue to drill 5mm inside and outside, and drill longitudinal holes in the back, which is conducive to the next osteotomy;
e: After osteotomy along the original drill hole, move the lower bone cortex down to leave a bone trough;
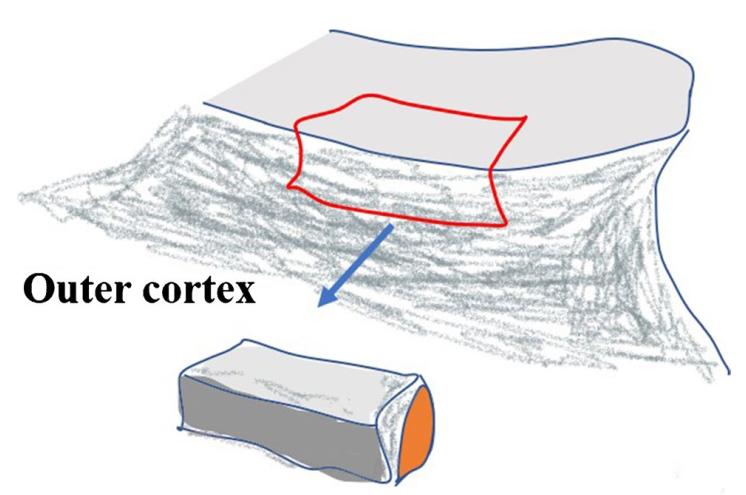
f: Bicortical iliac bone was implanted in the bone groove, and then the upper cortex, the iliac crest and the lower cortex were fixed with screws; The iliac cancellous bone was inserted into the fracture space
Typical
cases:
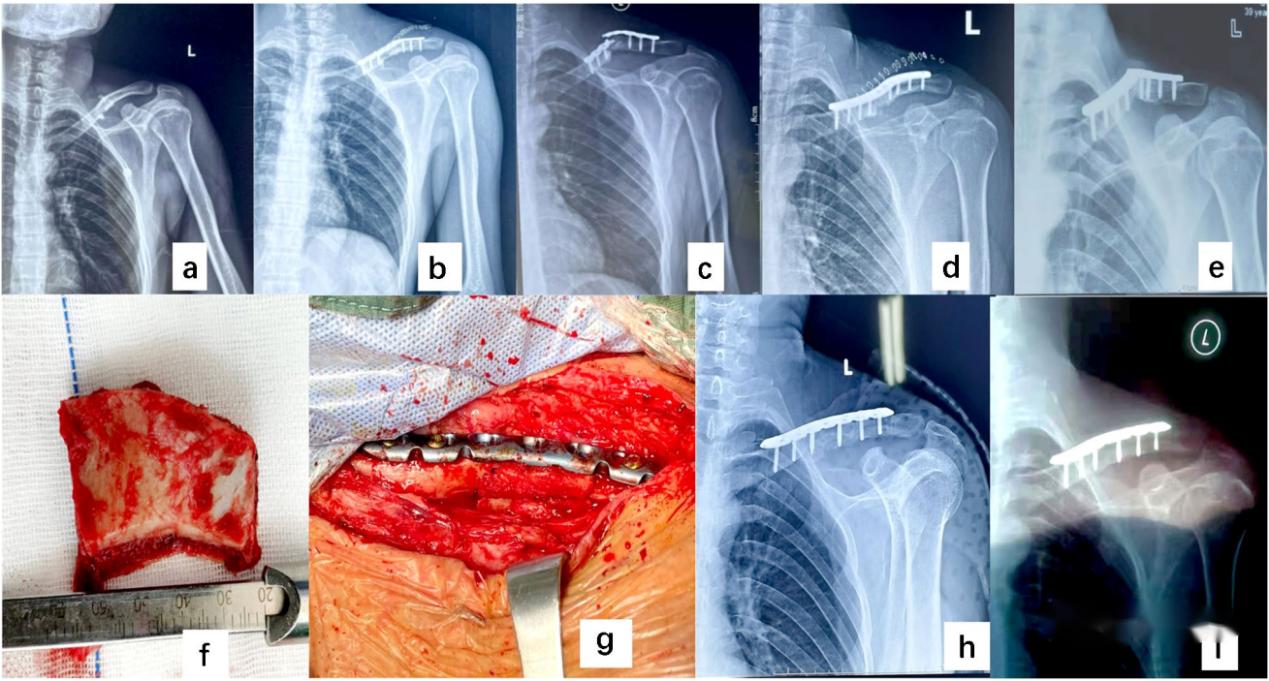
▲ The patient was a 42-year-old male with a mid-section fracture of the left clavicle caused by trauma (a); After surgery (b); Fixed fracture and bone non-union within 8 months after surgery (c); After the first renovation (d); Fracture of steel plate 7 months after renovation and non-healing (e); The fracture healed (h, i) after structural bone grafting (f, g) of the ilium cortex.
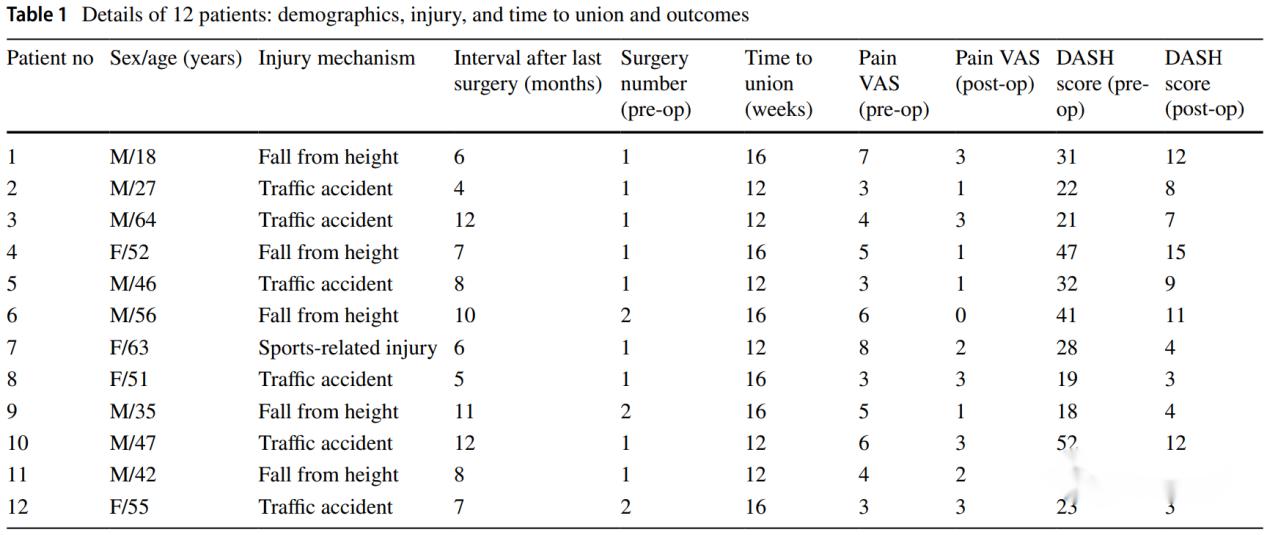
In the author's study, a total of 12 cases of refractory bone nonunion were included, all of which achieved bone healing after surgery, and 2 patients had complications, 1 case of calf intermuscular vein thrombosis and 1 case of iliac bone removal pain.
Refractory clavicular nonunion is a very difficult problem in clinical practice, which brings heavy psychological burden to both patients and doctors. This method, combined with structural bone grafting of cortical bone of the ilium and cancellous bone grafting, has achieved a good outcome of bone healing, and the efficacy is accurate, which can be used as a reference for clinicians.
Post time: Mar-23-2024





